Lasik is currently the best
method of correction of refractive errors. It is
accurate, effective and safe.
In LASIK an ultra-thin (90 to 150 micron) flap of
cornea is raised and then using a computer
guidance Excimer Laser (mostly Argon Fluoride 193
nm) is delivered to reshape the corneal stroma into
predetermined curvature. The flap is repositioned
back. This leads to correction of myopia,
hypermetropia, and astigmatism. The procedure is
short and simple and being computer controlled is
highly accurate.
Case selection is an
extremely important determinant of the results of
Lasik surgery:
Refractive error: -1.50
to -10.0 diopter of myopia or up to +6.0 diopter
hypermetropia (in patients older than 40 years
Lasik is not beneficial for low myopia of up to
-3.0 D)
Aberrometry to measure
higher order optical aberrations
Pupillometry to measure
pupil size in low light conditions
Intra-Ocular Pressure (IOP)
measurement
Detailed Retina
Examination
Informed consent
Antibiotic eye drops to
be instilled for about 2-5 days before surgery
Contact Lenses should be
discontinued for at least 2 weeks (Soft Lenses)
/ 4 weeks (Rigid Lenses) before the surgery
Lasik Procedure (see Video)
LASIK is performed under
topical anesthesia (Proparacaine Eye Drops) and the
only cooperation required of the patient is to
fixate at a blinking (green) light. Current LASIK
machines have an advanced eye tracker device which
realigns the Laser to any changes in the position of
the eye thereby ensuring proper centration of
ablation. The steps are:
After the anesthesia the
face of the patient is covered with a drape just
exposing the eye and an eyelid speculum is
applied to retract the eyelids (patient feels a
stretch on the lids). The patient fixates his
gaze at a blinking (target) light.
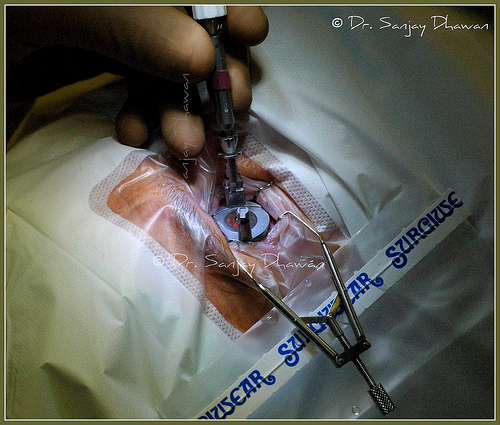
A suction ring is placed
around the cornea and serves to stabilize the
eyeball and act as a platform for the
microkeratome. When suction is activated vision
be comes hazy and a pressure on the eye is felt.
Pressure in the eye builds up and is measure to
ensure proper level.
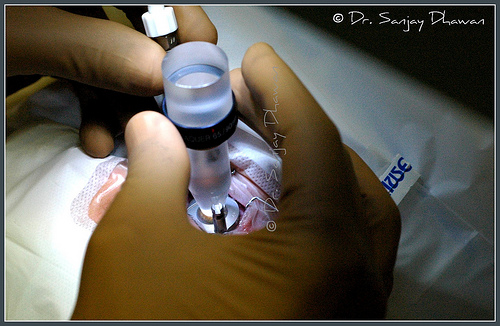
The automated
microkeratome dissects through the superficial
layers of the cornea and the corneal flap is
folded back. During this step the patient hears
the sound of a motor in front of the eye.
Then the flap is lifted and turned back to lye
on flap rest.
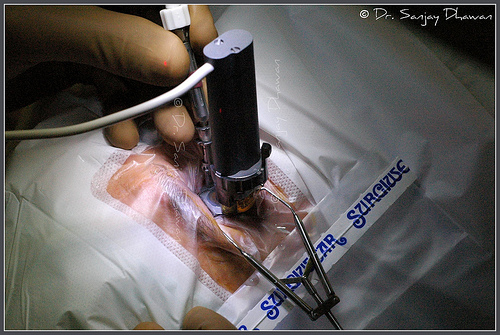
Excimer Laser ablates
the stromal bed to resurface it into desired
curvature. What makes the Excimer laser so well
suited for corneal ablation is its ability to
remove tissue with accuracy up to 0.25 micron
with each pulse. Often, only 50 microns of
tissue are removed to achieve the proper amount
of correction. The Excimer produces a
non-thermal light beam that eliminates the
possibility of thermal damage to surrounding
tissues. In current Lasers employing flying spot
technology a 1 mm spot ablates the tissue to
correct the refractive error and to blend this area with surrounding cornea by
creating smooth transition zones.
During this step a clicking / crackling sound is heard and
an odor of ablating tissue (similar to charring
hair) is smelt and a light flashing close to the
eye is seen. All this while patient needs to
concentrate on the center of the blinking
(target)
spot of light.
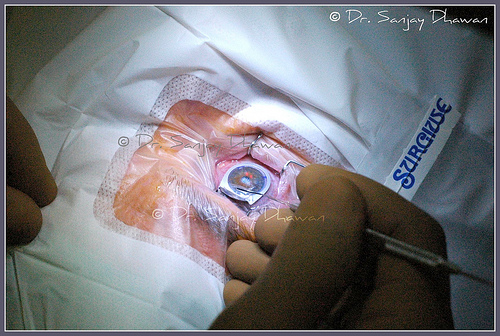
The corneal flap is then
repositioned and allowed to dry for a few
minutes. The flap self-seals without the need of
sutures.
Antibiotic drops are
instilled and the patient needs to rest with
eyes closed for about an hour before the patient
is discharged from the hospital. The patient is
advised to report back the next day. Eye drops
are prescribed to be started on the same day.
Analgesics are rarely required and that too for
1-2 days.
Lasik Surgery is
painless and the patient only feels slight
stretch on the eye lids and mild pressure on the
eye.
Precautions to be taken after Lasik
Avoid swimming and
splashing of water on the eyes for a month.
Avoid rubbing the eyes
for a month.
Use sunglasses to avoid
bright sun, dust, wind and air pollution.
Avoid excessive viewing
of TV or computers for a week.
Use medicines regularly
as advised. Lubricant or artificial tears eye
drops may be required for about 2-6 months
Consult your eye surgeon
in case of any problem
Avoid eye makeup for 1-2
weeks
Complications of Lasik
No surgical procedure is
without any complications. However, LASIK is a
relatively safe technique of correction of
refractive errors. The possible complications can
be:
Dry Eye
Under or over correction
Reduced contrast
sensitivity
Glare
Decentration of ablation
Astigmatism
Flap damage
Button holing of flap
Free Cap
Corneal perforation
Central Island
Infection
Corneal infiltration
Corneal Ulceration
Diffuse Lamellar
Keratitis (DLK or Sands of Sahara)
Corneal Ectasia
(Keratoconus)
Results of Lasik
Results are generally very
satisfactory and it has been reported that in
carefully selected cases more than 90 % achieve
unaided visual acuity of 6/12 or better (i.e., 6/12
6/9 6/6 6/5).
There is a subjective difference in degree of
satisfaction among the patients. Some patients with
a vision of 6/12 may feel very happy while others may
be dissatisfied even with a vision of 6/5.
It is important to discuss with your surgeon about
the expected results or prognosis in your case. Your
surgeon will be able to explain the kind of results
or problems likely in your case. A detailed
discussion helps a lot in preparation for Lasik.
Standard Lasik involves assessment of only refractive errors (myopia, hypermetropia or astigmatism) and correction of the same. But human eye may have some finer degrees of optical imperfections called aberrations. Standard Lasik does not correct these aberrations and may actually induce some aberrations leading to decrease in contrast and problems with low light conditions and night vision.
Wavefront guided or custom Lasik measures aberrations present in the eye (aberrometry) and attempts to correct them. Moreover, the treatment maps generated are customized to the individual eye and maintain the natural prolate profile of the cornea. This prevents induction of any aberrations. All this leads to better contrast and night vision.
Before the surgery it is important to dilate the
pupil of the eye with use of various eye drops which
may take about 1-2 hours.
The surgery is quite painless, however, the patient
may feel some pressure & touch on the eye. Patient
needs to stare straight up into the bright light of
the microscope through.
Epi-Lasik or Lasek
In patients with thin
corneas it may help to lift just a thin epithelial
flap as in Epi-Lasik or remove epithelium using
alcohol as in Lasek. This leaves behind greater
amount of tissue in the coneal bed to achieve higher
refractive correction.
Although it possible to correct greater amount of
refractive error in these procedures but the
recovery is rather slow and more uncomfortable than
in Lasik and there are greater chances of
development of corneal haze and regression.
Femtosecond Laser or
Intralase for Creating Flap ("No Blade" or
Blade Free Lasik)
Femtosecond Laser is a new method of creating
corneal flap in Lasik - here instead of
Microkeratome "Blade" or Disposable Microkeratome
Head, a Laser is used to cut the corneal flap.
Although it is touted as "No Blade" technique but
that should not mean that there is no cutting of
cornea to make a flap. The advantage is that the
flap reproduceability is better i.e. there is less
variation in flap thickness from patient to patient.
This variation is slightly more in Disposable
Microkeratome Head and significantly more with
Reusable Heads & Blades. However, there are reports
of increased risk of complications like DLK (Diffuse
Lamellar Keratitis or Sands of Sahara) caused by
disintegration of corneal tissue & collateral
damage. The newer ultrathin 90 micron disposable
microkeratome heads offer all the advantages of
Femtosecond Laser without an increase risk of DLK.
All these are relevant in thin corneas or high
refractive errors where one is working close to the
limits of safety.
SBK (Sub Bowman's
Membrane Keratomileusis)
In thist ype of Lasik
Surgery an ultrathin flap of 110 micron is created
lifting only the epithelium & Bowman's membrane
layers of Cornea. As result more tissue is left in
the corneal bed providing strength to the eye after
surgery and preventing complications like ectasia or
keratoconus.
Time Involved
An optimal time schedule is
as follows:
Day 1 - Detailed eye examination (2 hours)
Day 2 or 3 - Lasik Surgery (3-4 hours in the center
/ hospital)
Day 3 or 4 - First post-Lasik examination (1 hour)
Day 7-10 - Second post-Lasik examination (1 hour)
Patient may return after the second examination and
follow-up with local eye care practitioner every 2-4
weeks for 3 months.
Discussion: Standard Lasik vs. Custom Lasik
What is standard Lasik & what is custom Lasik? Which
is better for me & why? I am often asked this
question by my patients.
Standard
Lasik
This is the conventional type of Lasik Laser where
only the refractive error (myopia, astigmatism or
hypermetropia) is taken into account in the Laser
protocol and corrected.
This type of Lasik treatment does not correct
aberrations (finer optical defects in the eye) and
may actually increase them.
Custom Lasik
In this Lasik treatment in addition to refractive
error, finer optical aberrations are also taken into
account. The Laser ablation protocol attempts to
correct the aberrations as well.
The information about the aberrations in the eye is
provided by an instrument called aberrometer which
forms an additional link in the treatment chain.
Which is better & why?
High levels of aberrations in the eye adversely
affect contrast and night / low light vision. So if
aberration level is high (RMSh > 0.25) then
certainly Custom Lasik is better as it provide
better quality of vision, better contrast and better
night vision by correction of aberrations along with
the refractive errors.
If the aberration level is low (RMSh < 0.25) then
Custom Lasik is not really required and standard
Lasik works as well.
It may be noted that the vision in bright day light
is the same after both forms of Lasik (standard or
custom) and it's only in mesopic or low light
conditions that there is a difference in the quality
of vision. And the difference is very subtle & mild
- not a dramatic difference
Conclusion
LASIK is major advance in
the field of refractive surgery, which combines
efficacy, safety, precision and accuracy. This
technique is taking us on the path that, in the
past, ophthalmologists feared to tread, towards the
goal of unaided natural clear vision. However, it is
prudent to have realistic expectations from this
surgery and never hope for miracles (although
results of Lasik are no less).
Author: Dr. Sanjay Dhawan
Last Updated on: 1 March, 2014